Oxygen Therapy: The First 150 Years (continued)
1908
OXYGEN IN MEDICINE AND SURGERY -- A CONTRIBUTION, WITH REPORT OF CASES, by William Seaman Bainbridge, M.D., New York City. New York State Journal of Medicine, Vol. 8, No. 6, June 1908, pages 281-295. [This review includes a brief history of oxygen therapy, a rendition of who was making oxygen in New York and by what method at the time, and its current usage. Dr. Bainbridge's main emphasis, however, is his work on abdominal administration of oxygen; this route probably did help in selected cases. In the first two decades of the 20th century there were numerous papers about ntra-abdominal, intravenous, rectal, and subcutaneous administration of oxygen.]
|
. . . to Priestley may be given the credit for initiating the experiements which have called forth the extensive, if more or less chaotic, investigation recorded in the literature of the subject. . . . The first experiments on human beings are said to have been made by Chaussier, in 1783, in cases of dyspnea in consumptives and in asphyxia in infants. In the same year Caillens reported the cure of two cases of consumption by oxygen inhalations. In 1789 Beddoes, professor of Chemistry at Oxford, and a physician of repute, detailed his experiences and formulated his conclusions. It appears that he employed oxygen and other gases in his "Pneumatic Institute". . . [see 1789 in this chronology.] . . .from a review of the literature and from personal observation of the work of my colleagues here and elsewhere, the solution of the problem of the therapeutic value of oxygen is still inchoate. The failure of the medical profession to grapple with the subject in a definite manner was at first due, no doubt, to the difficulty experienced in the production of the gas in sufficiently pure state for purposes of inhalation. . .and in its transportation to the bedside of the patient. . . .Despite the laudatory claims for oxygen by the advocates of the "Home Treatment," the "Oxygen Parlor," the "Oxygenized Air," the "Ozone," et cetera, and despite the mass of clinical data recorded with favorable comment, the one hundred and thirty five years which have elapsed since the discovery of this gas have not given it a definite and unquestioned place in the realm of medicine. The chief methods for the therapeutic employement of oxygen are by inhalation, subcutaneous injection, intravenous infusion, introduction into smaller body cavities, especially the joints, and the introduction into larger body cavities (pleural and abdominal). [Dr. Bainbridge then discusses at great length his own work on abdominal administration of oxygen, providing numerous cases. One is quoted below.]
CASE VIII. M.G., age 49, single. Cystic ovaries and fibroid tumor of uterus, chronic appendicitis, and large cystic left kidney. Operation, New York Skin and Cancer Hospital, December 7, 1907. Through abdominal incision diseased kidney, appendix, ovaries, tubes, and uterus removed. Cyanosis marked. Shock very great, particularly at time of removal of uterus. Oxygen administered intra-abdominally, immediately following which patient's condition was greatly improved, pulse became stronger, blood brighter and more scarlet, cyanosis disappeared, and general condition of patient improved. Recovery uneventful.
|
1910
THE THERAPEUTIC USE OF ALCOHOL VAPOUR MIXED WITH OXYGEN, by W.H. Willcox, M.D., F.R.C.P., St. Marys Hospital, London, and Professor B.J. Collingwood, M.D., Professor of Physiology, the Catholoic Univesity School of Medicine, Dublin.[Alcohol was a popular stimulant in medical therapy, so it seems only natural that someone would mix it with oxygen.]
|
The combination of oxygen and alcohol vapour was first used in some experiments on animals made by one of usin 1907, in which it was found that after an overdose in chloroform anaesthesia the mixture of oxygen and alcohol vapour was a very valuable remedy for the cardiac failure which had wupervened as the result of a toxic dose of chloroform. It was found that the effect of oxygen containing alcohol vapour was greater than that of oxygen alone.As a result of these experiments oxygen which had been bubbled through absolute alcohol contained in an ordinary wash-bottle was administered by one of us in several cases of illness in which cardiac failure was a prominent symptom, and it was found that the mixture produced a remarkable stimulant effect on the heart and circulation decidedly greater than that produced by oxygen alone. In some of these cases the administration appaered to have been the cause of the prolongation and saving of life. [After further extensive discussion of the subject, and the reports of some very limited experiments, the authors offered the following CONCLUSIONS.] 1. The administration of oxygen bubbled through absolute alcohol is a marked cardiac stimulant in cases of heart failure. 2. The administration is pleasant and non-irritating in the the patient; it causes no ill effects to the lungs or bodily system. 3. A rapid feeble pulse is slowed by some 10 or 20 beats per minute, and there is a marked improvment in its force and volume. The blood pressure, if low from cardiac failure, is raised from 10 to 30 mm. of mercury. . . 4. It is better to use absolute alcohol in the wash bottle, since with less concentrated froms of alcohol an insufficient amount of alcoholic vapour will be contained in the oxygen. 5. The oxygen should be bubbled through the alcohol in a rapid stream. 6. The full effect of the administration is obtained after five minutes, and lasts for several minutes afterwards. As the effect passes off the administration should be repeated. |
1912
THE ADMINISTRATION OF OXYGEN, by Leonard Hill, M.B., F.R.S., Lecturer in Physiology, London Hospital Medical School. The British Medical Journal, January 13, 1912, pages 71-72. [The purpose of this short article was to introduce a specially-designed mask that delivers a high concentration of oxygen. However, the article is interesting mainly for the perspective Dr. Hill provides on oxygen delivery methods of the era; he minces no words.]Oxygen is usually given in a thin stream through a nozzle or small funnel held more or less near the mouth or nose of the patient. I have seen a nurse hold it 6 in. away. This method is more than ineffcient; it is absurd. The oxygen diffuses into the atmosphere, and the patient inspires air enriched very slightly with oxygen. Analyses of the pulmonary alveolar air -- obtained from subjects to whom oxygen was administered in this way -- showed an increase of only 1 to 2 per cent. If a most wasteful current was used and the funnel held close to the mouth, the increase was at most 10 per cent. . .. . .Ludicrously inefficient as the nozzle and funnel methods are, I have known of a practitioner going a step further in absurdity, in allowing the oxygen to escape in the patient's room! A man might as well hope to affect the composition of the sea by emptying his bladder into it. It has been ascertained that in places situated at high altitudes, such as Mexico City, it gives the patient who has pneumonia much the better chance if he is rushed down to the plains. |
1914
THE SUBCUTANEOUS INJECTION OF OXYGEN GAS, by H.O. Howitt, M.D., L.R.C.P. (Lon.), M.R.C.S. (Eng.), Guelph. The Canadian Medical Association Journal, 1914, Volume 4; pages 983-985. [This article, plus the papers by Kellogg (1888), Bainbridge (1908), Tunnicliffe & Stebbing (1916) highlight non-inhalational methods of giving oxygen. The two principle drawbacks of all these methods are their non-continuous administration, and the fact that most of the oxygen entered the venous circulation. However, the nature of the case reports in this 1914 paper indicates that, as Dr. Howitt claims, SQ administration does appear to help -- and certaily not hurt -- in urgent situations.]Every pracitioner finds some time or other the giving of oxygen to be indicated as a therapeutic measure, and he give it -- with results so indifferent that beneficial effects are invariably of note only by their absence.. . .Delmas and Delmas in 1912 reported excellent success in resuscitating asphyxiated infants by this method. Derose recommends the use of oxygen by the subcutaneous method in cases of tuberculosis with dyspnoea, and remarks that "the temperature falls and a feeling of well-being immediately prevails, for which the patient is very grateful, and sleep, previously impossible, becomes soothing and refreshing." He suggests its employment for 1) the toxic dyspnoea of uraemia, 2) eclampsia, 3) carbon di-oxide poisoning, 4) in certain cases of diabetes, 5) emphysema, 6) pertussis, 7) asystole, and 8) in those cases where mechanical obstruction is precisely located in the air passages. My experience, which now covers nearly two years, includes the dyspnoea of tuberculosis, gas poisoning, pneumonia (lobar and lobular), oedema of the lungs, bronchial asthma, and operative cases. In no case were any ill effects noticeable, either at the time or afterwards. One asthmatic said that it relieved him, but did not notice appreciable improvement. The carbon di-oxide case may have recovered without the injection, but in some of the pneumonia and operative cases the results were simply astounding. [Dr. Howitt presents 6 cases, one of which is quoted below.]
Case 2. A woman, sixty-six, with lobar pneumonia; temperature 103 1/2 degrees, respirations forty-six, rapid pulse, rusty sputum. The condition became alarming on the fourth day from the onset. Oxygen was injected. The temerature dropped a degree, and almost at once the breathing became less laboured, and the patient was very grateful. Injections were given twice daily, and the case no longer resembled pneumonia.
. . .The following is a description of the apparatus and the method of its use: Oxygen is generated from sodium peroxide coming in contact with water in a closed cylinder, and the gas set free escapes by means of a long rubber tube, at the distal end of which is an aspirating needle which is inserted into the subcutaneous tissue. The tube is then oiled and by a pumping action of the hand, sufficient force is used to raise a lump once or twice as large as the closed fist. The oxygen injected by this method forms a local emphysema which lasts for hours and may travel over the surface of the body. Apparently the body only absorbs that which is necessary. It is really the formation of an artificial lung. I have never known a single ill effect to follow its use; in every case where the breathing was labored, the patient experienced some relief. . . It is not a "sure cure" for pneumonia or any other disease, but when oxygen is urgently needed by the cells of the body this method of introduction of oxygen fills the requirement. In my experience the old method of inhalation was a failure.
|
1916
THE INTRAVENOUS INJECTION OF OXYGEN GAS AS A THERAPEUTIC MEASURE, by F.W. Tunnicliffe, M.D., Lond., & G.F. Stebbing, M.B., B.S., Lond. The Lancet, August 19, 1916. Pages 321-323. [Another example of the administration of oxygen by non-inhalation methods; see also Kellogg (1888), Bainbridge (1908), Tunnicliffe & Stebbing (1916).]For some time it has been the practice of one of us (Tunnicliffe), when using saline venous injections, either simple nutrient (glucose and lecithin) or medicated, to use not simple saline solution but oxygenated saline solution. We are quite aware that the quantity of oxygen introduced by this method is very small as compared with the oxygen requirement of the subject, nevertheless cyanosis is rapidly alleviated by the use of such solutions, and we have observed that more rapid and generally better results are also produced by such (oxygenated) solutions quo their nturitent and medicinal content than by similar solutions, the bsais of which is simple saline solution. . . .The object of this preliminary note is not to indicate the specific pathological conditions in which the intravenous injection of oxygen should be used, but simply to point out that in those cases in which the inhalation ofoxygen either cannot be practised or gives inadequate relief, the intravenous method of oxygen administration, if carefully carried out in accordance with the above, is available to the clinician and will give therapeutic results. |
1917
THE THERAPEUTIC ADMINISTRATION OF OXYGEN, by J.S. Haldane, M.D., F.R.S. British Medical Journal, February 10, 1917, pages 181-183. [The modern era of oxygen therapy began after World War I, with publication of Haldane's experience in treating war gas injuries. Although methods of oxygen measurement remained unavailable for many years afterwards, this paper is considered to mark the beginning of modern oxygen therapy.]
It is well known that the administration of oxygen often produces at least temporary benefit in cases of serious interference with the respiratory or circulatory functions; but sufficient attention has not hitherto been paid either to what precise benefit may be expected from the administration of oxygen, or to how it can best be administered. In the present paper I propose to discuss both these questions in light of existing physiological knowledge, and to describe an apparatus designed for the clinical administration of oxygen. Our knowledge of the physiology of respiration has advanced very rapidly within the last few years, and certain points which have been elucidated in this advance must first be adhered to.. . . . .Where, in lung affections, an addition of oxygen to the inspired air is needed in order to combat want of oxygen, it is evidently desirable to continue the administration over long periods. . . In cases where the source of danger is failure of the circulation, the inhalation of oxygen may also be of use, and I have seen the cyanosis in a case of valvular disease clear up at once on the administration of oxygen. . .
. . .The probable risks of prolonged administration of pure oxygen must be borne in mind, and if necessary balanced against the risks of allowing the oxygen want to continue. No fixed rule can be given. The proper course to pursue must be determined by the physician after careful observation of the patient, and in the light of experience and knowledge. . . |
1917
THE THERAPEUTIC VALUE OF ORAL RHYTHMIC INSUFFLATION OF OXYGEN, by S.J. Meltzer, M.D., LL.D., New York. Journal American Medical Association, October 6, 1917, pages 1150-1156. [One of the earliest articles to discuss the therapeutic value of oxygen delivered under positive pressure. Meltzer's patients received what today we would call IPPB, or intermittent positive pressure breathing. Oxygen was allowed to enter the upper airway under pressure from the oxygen tank, 12 times a minute. Unfortunately, like much of oxygen therapy at the time, this "rhythmic insufflation" was only administered a few times a day. The concept of continuous need was still not widely accepted. The last sentence quoted shows Dr. Meltzer was aware of the benefits of positive pressure breathing.]
|
Two factors are at the bottom of the skeptical attitude of physicians toward the value of oxygen as a therapeutic agent. In the first place, many clinicians are influenced by the view entertained by the great majority of physiologists that the addition of oxygen to the inhaled air is incapable of exerting a physiologic influence, that it does not affect the metabolism, and that the added oxygen returns unabsorbed. [To counter this assertion, Dr. Meltzer quotes Haldane's paper that appeared earlier in the year - see above. He then continues:]
. . .probably the more influential factor, is the actual fact that practitioners rarely see any favorable effect that may have been brought about by the administration of oxygen. . .The failure to see such an influence is probably due essentially to the inefficient method of administration. In most instances oxygen is given in a weak current through a funnel which is kept an inch or more from the mouth of the patient. Under these conditions we can hardly speak of "inhalation of oxygen." The atmospheric air which the patient actually inhales is probably not richer by more than 2 per cent. of oxygen, if by so much.On the other hand, the funnnel may be instrumental in making the inspired air richer in corbon dioxid [sic] and surely makes the air over the face warmer, an unpleasant sensation to the patient, who prefers to be fanned and cooled off. Therefore, we often see the patient pushing the funnel away or turning the head away from it. [He then describes a 25-year-old man dying with pneumonia]. . .
Nurses were administering oxygen in the usual manner, that is, through a paper funnel, kept at some distance, the gas bubbling through a wash bottle at a moderate pace.
I disconnected the rubber tube from the foot bellows of my pharyngeal insufflation apparatus that I brought along with me, and connected it with an oxygen cylinder. I then inserted the pharyngeal tube in the mouth (not in the pharynx), turned on the oxygen and started working the respiratory valve. [As described in the article, the valve referred to, when open, lets oxygen flow through the tube under tank pressure; when the valuve is closed, the flow of oxygen is cut off. The valve is opened and closed 12 times a minute.]
Within a short time after the beginning of the oxygen insufflation in the new manner, the cyanosis disappeared and the face of the patient became actually pink. Several minutes after the discontinuance of the insufflation, the cyanosis began to reappear gradually. In the course of the next five hours the experiment was repeated numerous times and invariably with the same result, that is, the cyanosis disappeared promptly during the insufflation of oxygen and reappeared several minutes after cessation of the insufflation. . .The patient was not saved; but nobody could have expected it when beginning treatment at that terminal stage.
...I have tested on myself the action of insufflation of oxygen by means of this apparatus. When the insufflation is carried on under moderate pressure, there are no unpleasant sensations whatever. When it id done under too much pressure, the surplus of oxygen escapes through the nose and never enters the esophagus; but it causes some unpleasant sensations which conscious patients will probably not be willing to stand for any length of time. My chest was examined by auscultation while I was receiving oxygen insufflation. It was found that each insufflation produced a distinct inspiratory blowing sound which was distinctly recognized even while I was holding my breath. It seemed, further, that the oxygen was capable of entering my lungs even when I was endeavoring to keep the glottis in a state of adduction. . . . . .it must be admitted that the rhythmic insufflation, since it is capable of assisting in the maintenance of the respiration, may be helpful in the ventilation of the lungs and thus helpful also in the removal of some of the accumulated carbon dioxid. |
1920
REPORTS OF SOCIETIES: OXYGEN THERAPY. A discussion on the therapeutic uses of oxygen, January 20th, 1920, in the Section of Therapeutics and Pharmacology of the Royal Society of Medicine, including comments by J. Barcroft and J.S. Haldane. British Medical Journal, January 31, 1920. [In this paper an unnamed moderator tells of the "discussion," which included eminent scientists J. Barcroft and J.S. Haldane. Of note is the rapidity of publication in the BMJ, 11 days between the meeting and the printed report. This paper shows the definite trend toward "science" in oxygen therapy and away from mere conjecture and anecdote. Haldane spoke directly to the physiology of hypoxemia, i.e. diffusion impairment and ventilation-perfusion imbalance. (The American W.C. Stadie, mentioned by Haldane, did the first measurements of oxygen saturation in pneumonia.)]
The discussion was opened by Mr. J. Barcroft, C.B.E., F.R.S., who said that the subject of oxygen therapy was no new one, and it had now reached a stage at which there was considerable diversity of opinion. In such circumstances the best method of treating a subject was to produce facts, and the work of himself and his colleagues had been on those lines. His work on oxygen therapy had been limited to the treatment of a particular class of case - namely, soldiers and munition workers who had been gassed. . . The method adopted at Cambridge was simple.
A glass room of about 1,000 cubic feet capacity formed a living ward and contained three beds. The ward was gas-tight and fitted with air locks. The composition of the atmosphere within was kept at 40 to 50 per cent. of oxygen and 50-60 per cent. of nitrogen. The CO2 and aqueous vapour were removed by passing the air from the ward through an external circulit containing scrubbers of soda-lime and calcium chloride and potassium permanganate.
. . . In the first fourteen cases studied they took the response of the pulse to effort as the criterion; in the last twelve the respiratory response. . .
A typical case was that of S., gassed April, 1915, presumably with chlorine; treated October, 1917. Pulse before treatment took nine to ten minutes to fall within six beats per minute of resting rate after test exercise. After treatment it returned in the fourth quarter minute. . .
[Dr. Haldane] wished to emphasize two points: 1) That very slight anoxaemia had a very serious effect if persisting for a long time. For example, seriously unpleasant symptoms of mountain sickenss often followed exposure for some hours to slight lowering of th eoxygen pressure of the atmosphere. The same effect followed slight CO poisoning, and the serious symptoms were apt to be delayed and come on after the cause provoking them was no longer operative. 2) That anoxaemia was very common in acute illnesses. In such cases it was desirable to prevent the anoxaemia and to do so at an early stage. . . A reliable method of detecting slight degrees of anoxaemia was to administer oxygen and note any resulting change of colour. If anoxaemia were present the lips would become redder. The occurrence of anoxaemia in acute illnesses was well shown by recent work in America. Stadie had analyzsed the gases of arterial blood in cases of pneumonia, etc. Nearly all showed a deficiency in the degree of saturation of the blood with oxygen, which might amount ot as much as 50 per cent. in some cases. Such cases with only half the normal amount of oxygne in the arterial blood all died. Similar results were obtained in heart disease and bronchitis. Anoxaemia (deficiency of oxygen in the arterial blood) might be due to two causes.
1. Thickening of the alveolar epithelium of the lungs. 2. Unequal ventilation of different parts of the lungs.
. . . After the meeting Dr. Haldane demonstrated the apparatus devised by him for the administration of oxygen. |
1922
RESPIRATION, by J.S. Haldane. [This 427 page book contains the state of the art on respiratory physiology as of 1922. Haldane discusses oxygen and carbon dioxide transport, the nervous control of breathing, effects of low and high atmospheric pressures, and many other topics. The title page is reproduced below, and brief quotes are provided from the Preface and Chapter VII, the latter pertaining to oxygen therapy.]
RESPIRATIONBYJ.S. HALDANEM.D., LL.D., F.R.S.FELLOW OF NEW COLLEGE, OXFORDHON. PROFESSOR, BIRMINGHAM UNIVERSITY
NEW HAVENYALE UNIVERSITY PRESSLONDON:HUMPHRY MILFORD:OXFORD UNIVERSITY PRESSMDCCCCXXII-------------------------------------------------PREFACE. . .The book is not a mere compilation, but contains much that has never previously been published, and is an attempt to give a coherent statement and interpretation of what is known of the subject at present. . .The keynote of this book is the organic regulation of breathing and its associated phenomena. . . -------------------------------------------------[from CHAPTER VII. The Causes of Anoxemia; pages 151-152.] . . .In the great majority of cases, however, the cause of the anoxaemia is one which may last for a considerable period of time, so that the administration of oxygen, in order to be useful, must be continued. In this connection it should be clearly realized that the object of the oxygen administration is not simply palliative, but curative. By preventing the anoxaemia we not only avert temporarily a cause of danger or damage to the patient; but give the body an interval for recovery from the original cause, whatever it may be, of the anoxaemia, or for adaptation. We also break a vicious circle: for if the anoxaemia is allowed to continue, it will itself make the patient worse, or tend to prevent the recovery which would otherwise naturally occur. We are not dealing with a machine, but with a living organism; and a living organism always tends to return to the normal if the opportunity is given. Oxygen is still often given by methods which are either quite ineffective or extremely wasteful. One method is to place a funnel over the patient's face, and allow some quite indefinite amount of oxygen to pass into the funnel. By this method the patient rebreathes a good deal of expired air, but may hardly get any of the oxygen, as the latter, being heavier, runs out below. A far better method is to insert a rubber catheter or other soft tube into the patient's mouth or nose, and pass a stream of oxygen through the tube. Another good method, when pure oxygen has to be given, is to allow the oxygen to pass at a sufficient rate into a rubber bag connected with the inspiratory valve of an anaesthetic mask placed over the patient's mouth and nose. The patient inhales from the bag, and exhales to the outside through the expiratory valve in the mask.
|
1928
From a news article of this period:
"One of the strangest experiments in medical science's long and constant fight against disease, an
experiment to which H.H. Timken, Canton, Ohio, manufacturer, has given $1,000,000, has been
undertaken in Cleveland, Ohio. It is the Timken Tank, a huge airtight, steel ball fitted out as a
hospital, in which patients suffering from diabetes and other maladies will live under 30 pounds
air pressure, which is forced into the steel ball by powerful compressors."
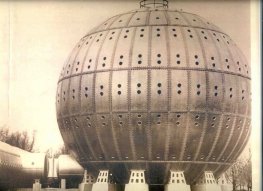
For more on this "Monster Steel Ball," as it was called, go to
Questions and Answers about the Monster Steel Ball.